

Hospitals Hit Back On Drug Pricing, But Will They Knock Out The Problem?
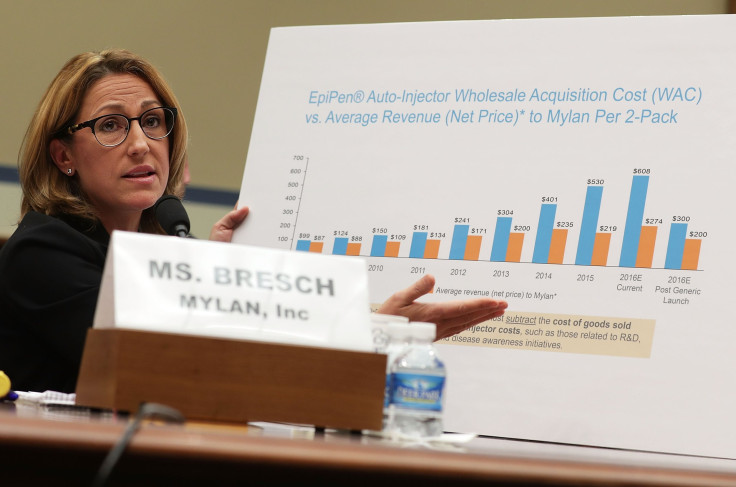
Drug manufacturing and pricing vaulted into the news several years ago when a privately held company raised the price of a drug used for infections from US$13.50 to $750 for one pill.
After an outcry from hospitals, the company later relented, dropping its price by a small margin. Still, this single dramatic increase shed light on the once obscure arena of older generic drugs that continue to be in short supply and whose prices occasionally skyrocket.
Frustrated with these shortages and alarmed by the potential for price gouging, a coalition of hospitals has recently struck back. Four not-for-profit, religiously affiliated hospital systems and the U.S. Veterans’ Administration announced their intent to form a company that would manufacture generic drugs, thereby helping to mitigate or eliminate shortages and prevent future massive price spikes for rarely used generic drugs.
I’m an economist who has studied the health care industry, including the U.S. generic industry, and I see a few regulatory and business hurdles to this approach.
Worthy Goal, But Challenges Aplenty
The formation of a generic drug company by not-for-profit hospital chains to address continuing drug shortages and mitigate periodic price spikes of old, rarely utilized generic drugs is understandable and reflects a worthy goal. It is important to realize, however, that there are reasons the markets for these old drugs are small. Most are unprofitable, and drug availability may not be guaranteed even if they are produced and marketed by not-for-profit organizations.
Three substantial challenges face the new generic company, each involving coordination clashes within the buying consortium. First, what specific generic drugs should the new generic company manufacture and market? A press release accompanying the announced collaboration suggested the consortium would market about 20 generic drugs.
But which generic drugs? Those drugs with the greatest price increases? Those whose shortages most threaten public health? Those critical drugs currently available, but whose possible price increases or supply disruption pose the potentially greatest threat to the public health? Those associated with the lowest production costs or least complex manufacturing? Given diverse preferences among its membership, the coalition may find it very difficult to reach a consensus on which generic drugs to manufacture.
Second, once a decision has been reached on which generic drugs to manufacture and market, the consortium must obtain regulatory approval from the FDA via the Abbreviated New Drug Approval process, either by reaching an agreement with an existing manufacturer with that approval, or by filing completely anew.
If the former, the consortium would need to utilize the identical manufacturing processes, facility sites and equipment as specified in its Drug Master File accompanying its original application for new drug approval. That would have to happen even if those manufacturing processes were now antiquated and inefficient given technological progress in biochemical manufacturing.
If instead the consortium decided to upgrade the manufacturing processes, then it would need to work with the FDA to satisfy regulatory bioequivalence requirements with the new equipment, a process that involves capital expenditures and can take several years. Bioequivalence means that there is no important difference in the rate and extent of absorption of the active pharmaceutical ingredient. In this latter case, it may instead be preferable to file a completely new application.
Even in that case, though, the consortium would need to decide whether it would self-manufacture the generic product or outsource it to a willing and FDA-acceptable contract manufacturing organization. Agreements and contracts would be required for each generic product, although it is possible that a single contract manufacturer could be identified who could manufacture several of the desired generic drugs. The process by which necessary FDA regulatory approval would be obtained would therefore involve drug-specific approvals and numerous contractual negotiations, consume a considerable amount of time and potentially require substantial capital investments.
Third, once decisions were made on which generic drugs to market and how they would be manufactured to ensure they satisfy FDA regulatory requirements, the consortium must determine how to store, distribute and price the medicines. If, given the prices charged by the consortium, the demand for the generic drugs exceeds available supply, how will the unsatisfied demand be rationed – by price increases, an algorithm based on members’ previous purchases from the consortium or by profit versus not-for-profit considerations? How to unload product if supply exceeds demand, generating unused inventories of old generic drugs?
It is possible, of course, that the newly announced generic consortium will be able to overcome coordination challenges and mitigate the market imperfections – and it is important that private, public and philanthropic organizations provide the consortium with various forms of support – but the challenges are indeed daunting. The ultimate success of this generic drug consortium initiative would be a wonderful development – but I wouldn’t count on it.
Ernst Berndt is a Professor of Management at MIT Sloan School of Management
This article originally appeared in The Conversation. Read the original article.
<img src="https://counter.theconversation.com/content/93826/count.gif?distributor=republish-lightbox-advanced" alt="The Conversation" width="1" height="1" />

- MOST READ



















